How the world went from no COVID vaccines to two in under a year
No vaccine in history has been developed this quickly.
First identified in 1545, smallpox ravaged humanity for centuries, spreading rapidly from India through Europe and into the New World. Smallpox is estimated to have killed 300 to 500 million people in the 20th century alone. But thanks to an unprecedented global vaccination program, smallpox has since been eradicated with no known natural cases reported since 1977. Today, we face another pandemic threat in the COVID-19 virus, which has infected nearly 70 million people worldwide and killed close to 1.6 million. So far, 293,000 of which have been American. Vaccines are being developed, but can the global community band together and mount a similarly ambitious effort to wipe out COVID as we did smallpox?
British physician Edward Jenner is credited with devising the first vaccine in 1796 when he inoculated a 13-year-old boy with cowpox material to create an immunity against its more deadly cousin, smallpox. Basically, the antibodies produced by the boy's immune system in response to the cowpox later protected him when exposed to smallpox. Jenner's discovery launched the field of vaccinology and over the next 200 hundred-plus years, researchers have developed vaccines for anthrax, cholera, tetanus, polio, malaria, rabies and dozens of other diseases.
Vaccines are produced in a variety of ways, either by weakening or inactivating the virus, using just part of the virus, or by providing the body with a bit of the virus' genetic code. Moderna's COVID-19 vaccine, for example, contains a bit of messenger RNA that codes for the spike protein found on the surface of the SARS-CoV-2 virus. When injected, the body's muscle cells use that RNA to produce copies of the protein spikes. These in turn instigate an immune response from the body priming the immune system to respond faster the next time it encounters the COVID protein.
Any vaccine in development must first undergo rigorous safety testing before it is approved for use by the FDA. The treatment molecule is first modeled using computer algorithms to estimate how it will interact with the human immune system, then tested on cell cultures. The next stage involves testing the vaccine on animals. Should it prove effective in animals, the vaccine enters Phase I trials with a couple dozen volunteers participating.
Phase II can run for up to two years and involve several hundred patients. Data gathered from these trials "can be used to determine the composition of the vaccine, how many doses are necessary, and a profile of common reactions," according to the CDC. Once proven safe and effective in phase II, the vaccine will be administered to hundreds or even thousands of patients as part of the multi-year phase III trials, which determine how effective the vaccine is in a large population. Only after the FDA is satisfied that the vaccine is safe can it be licensed for use by the general public.
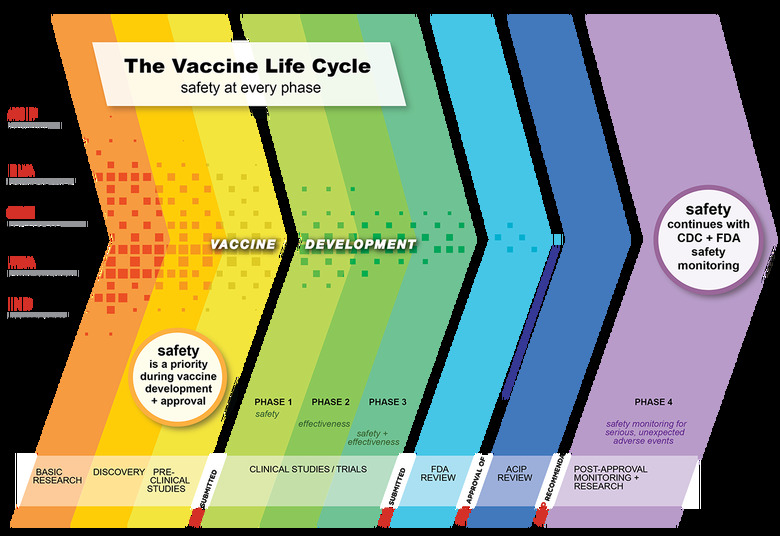
Earning FDA approval can take years to complete, which is why the government is currently allowing drug makers to apply for Emergency Use Authorization instead. In an effort to accelerate the vaccine development process while maintaining stringent safety testing standards, President Trump launched Operation Warp Speed (OWS) in May, 2020. This $10 billion initiative is a public-private partnership tasked with producing and distributing 300 million COVID-19 vaccine doses by January, 2021 as part of a broader federal effort to bring the pandemic under control.
"Rather than eliminating steps from traditional development timelines, steps will proceed simultaneously," per the HHS, "such as starting manufacturing of the vaccine at industrial scale well before the demonstration of vaccine efficacy and safety as happens normally. This increases the financial risk, but not the product risk."
Fourteen promising vaccine candidates were initially selected from a pool of hundreds for the Warp Speed program. Those have since been pared down to seven finalists, which are being developed in parallel at an unprecedented speed. No vaccine has ever been created in this little time.
This is amazing. December 2020. As late as this April, people—including Dr. Fauci—thought 18 months was probably too optimistic a timeline for vaccines. And we'd have been thrilled with ones much less efficacious than these. And multiple ones are in the pipeline. It is a triumph. https://t.co/g8y10YwFkN
— zeynep tufekci (@zeynep) December 12, 2020
For example, Moderna's mRNA-based vaccine, mRNA-1273, started out as a computer model in January, but within three months had already progressed to human studies. By November, just four months after beginning phase III trials, the company demonstrated its vaccine to be 94 percent effective in preventing COVID-19 infections. And among the participants who did contract coronavirus during the trial, none developed a serious case of the disease. The vaccine requires two injections spaced 28 days apart to maximize its efficacy, but be warned: The technology behind it is so new that researchers aren't yet certain how long its conferred immunity will last.
Moderna filed for FDA approval on November 30th and the agency's advisory board granted it emergency usage authorization on December 17th. It was the first time that an mRNA treatment has been approved for use against an infectious disease. But don't go lining up for your shots just yet: The company will only have a few tens of millions of doses available before it can ramp up production next year.
Pfizer, working in partnership with Germany's BioNTech, has shown similarly exciting results with its own recently authorized mRNA vaccine, BNT162b2, which earned FDA authorization on December 11th. Like Moderna's candidate, Pfizer's vaccine tricks the body into creating COVID-19 protein spikes and uses the resulting immune response to confer immunity. Of the 44,000 participants in Pfizer's phase III trials, which began in July, only 96 people contracted coronavirus. The clinical trial results are still preliminary — whether those 96 people were part of the vaccine or placebo groups has not been announced — but they do suggest that BNT162b2 could be more than 90 percent effective.
And the results are even more promising for vulnerable groups. As the LA Times points out, BNT162b2 prevented 95 percent of COVID-19 cases in both Latinos and non-Latinos, and 100 percent of Black people. It was also 94 percent effective in people over the age of 56, and 95 percent effective for people with an existing health condition that make them more susceptible to contracting the virus. That's a tremendous result given that the FDA only required COVID-19 vaccines be 50 percent effective when being submitted for emergency authorization consideration.
Pfizer has already gained authorization in the UK, the MHRA and the EU's EMA is set to announce its decision later in December. The company reportedly hopes to have 30 to 40 million doses available by the end of the year with initial deliveries arriving in the US on December 14th.
"Bringing it all together in a first-time, very large-scale operation, is no simple feat," Pfizer spokeswoman, Amy Rose, explained to The Washington Post. "It's as complicated as the research-and-development piece."
However, not every manufacturer's efforts have gone as smoothly. Researchers at the University of Oxford had already been working on treatments for MERS, a close relative of the COVID-19 virus, which made adapting to the new challenge a straightforward task, enabling the team to begin phase I trials in April. AstraZeneca subsequently signed on to handle licensing and manufacturing the tens of millions of needed doses. But in September, AstraZeneca ran afoul of US regulators after apparently failing to disclose to the FDA that the company had quietly halted trials worldwide just two days before requesting emergency authorization.
Less expensive to produce and more shelf stable than other coronavirus vaccines, the Oxford candidate was expected to constitute a large portion of the overall vaccine supply. But after dragging its feet for seven weeks in providing regulators with required documentation regarding the trial stoppages, AstraZeneca has fallen off the pace and has yet to finish enrolling people for its US trials — something the company repeatedly said it hoped to have ready by October. "The world bet on this vaccine," Dr. Eric Topol, a clinical trial expert at Scripps Research, told the New York Times in December. "What a disappointment."
The search for additional vaccine candidates continues. A study published in the journal Nature in December has identified five genes linked with severe cases of COVID-19: IFNAR2, TYK2, OAS1, DPP9 and CCR2. These genes, which are involved in antiviral immunity and lung inflammation, could help explain why some folks come down with coronavirus but remain asymptomatic while others end up in the ICU. More importantly, this identification can help guide researchers in finding new treatments. To date, only the steroid dexamethasone and Gilead's antiviral remdesivir have been approved to treat coronavirus patients.
"Our results immediately highlight which drugs should be at the top of the list for clinical testing," said Edinburgh University's Kenneth Baillie, who co-led the research, in an interview with Reuters.
But developing effective vaccines is only half the challenge. Ensuring that the vaccine is distributed equitably and efficiently is of critical importance but, as the OWS handout below illustrates, the process involves a lot of moving parts depending on which company is making it.
Handout from the White House on Operation Warp Speed ahead of a summit on vaccine distribution on Tuesday. pic.twitter.com/8vPrfci1GC
— Jeff Mason (@jeffmason1) December 7, 2020
To complicate the situation further, health officials around the country already anticipate a coming vaccine shortage struggle. The federal government has already announced it will stagger deliveries to states so that they can maintain a sufficient supply to administer the vaccine's second dose 21 to 28 days later. And despite the White House's repeated promises that a stockpile of 300 million doses would be assembled by the end of this year, the government is currently on pace to deliver only a tenth of that, around 30 to 40 million doses.
Officials in Maine, for example, were originally promised 36,000 doses but have since seen their allotment dwindle to only 12,675. Any potential shortages will hopefully be short lived and rectified come January and February as manufacturers ramp up production. Pfizer originally sought to produce 100 million doses by the end of the year but has had to revise that down to just 50 million in recent months. However, the company aims to produce 1.3 billion doses in 2021.
There are a number of factors that have hindered distribution efforts, from shortages of raw materials to manufacturing setbacks and difficulties in scaling production to a high enough level. "There were a couple of our vaccine candidates that took significantly longer, in terms of failed batches, in terms of not having the purity we sought," Paul Mango, HHS deputy chief of staff for policy, told The Washington Post earlier this month. "We have cracked the code on these things but we're two months behind on some of them."
Moderna, on the other hand, has been hindered by supply bottlenecks for the specialized materials used to create the vaccine. "The swing factor between 500 million and 1 billion [doses] is raw materials," Moderna CEO Stephane Bancel noted in a recent Washington Post interview. He explains that the company has already scaled up production by a factor of 1,000 in 2020. "Some of our suppliers were not ready for that, of course," he continued.
Despite these challenges, Operation Warp Speed chief adviser Moncef Slaoui remains optimistic that America will see a return to semi-normalcy by next Spring. "I think we may start to see some impact on the most susceptible people probably in the month of January and February, but on a population basis, for our lives to start getting back to normal, we're talking about April or May," Slaoui told a Face the Nation panel earlier this month.
Operation Warp Speed's Moncef Slaoui to @margbrennan on @US_FDA approval of a #COVID19 #vaccine: "Based on the data that I know, I expect the FDA to make a positive decision. But of course, it's their decision." pic.twitter.com/jfB3Z8q3BC
— Face The Nation (@FaceTheNation) December 6, 2020
Countering misinformation about the vaccine and convincing a skeptical public that it is indeed safe poses even more problems for health officials. A recently published study out of North Carolina State University suggests that our inflated opinions of our own ability to spot online misinformation better than other folks — known as the "third person effect" — plays a large part in misinformation's resilience.
The third person effect "makes it harder to get people to participate in media literacy education or training efforts," assistant professor of communication at NCSU, Yang Cheng, explained in a press release. "It suggests that most people think everyone else needs the training more than they do."
Of course, the Trump administration hasn't exactly done itself any favors on the topic of misinformation. The president has spent the weeks since November's election making unfounded claims about election fraud rather than participating in the transition process, which would enable the incoming Biden administration to seamlessly take over the fight against COVID-19. But, as such, President-elect Biden and his team have been largely kept in the dark about the current administration's pandemic response. It wasn't until the second week of December that Biden first had an opportunity to meet with OWS' Moncef Slaoui.
"We haven't had any meetings yet. I know we have a meeting this coming week and we really look forward to it because actually things have been really very appropriately planned," Slaoui said on Face the Nation earlier this month.
We plan to have all the ancillary material, the syringes, the needles, the swabs, everything co-localized with the vaccine. So, I think the plans are there," he continued. "And I feel confident that once we will explain it, everything in detail, I hope the new transition teams will understand that things are well planned."
In a separate interview with Fox News Sunday, Slaoui cautioned against getting complacent once the vaccine becomes available. "We all need to take our precaution, wear our masks, wash our hands, keep our distance, remain aware that this virus is a killer," he warned adding that there is "light at the end of the tunnel, but we will not all have the vaccine in our arms before May or June, so we need to be very cautious and vigilant."